 English
English 한국어
한국어 français
français Deutsch
Deutsch Español
Español русский
русский português
português العربية
العربية ไทย
ไทย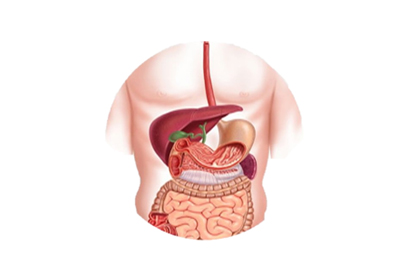

Address
1st & 2nd Floor, 10 Building, 18 Huashan Rd., Changzhou, Jiangsu province, China

Endoscopic retrograde cholangiopancreatography (ERCP) is a diagnostic and therapeutic minimally invasive procedure that involves inserting a duodenoscope through the mouth to the descending duodenum and entering the bile duct and pancreatic duct to perform imaging and other procedures. After more than 40 years of technical development, equipment updates, and clinical experience enhancement, ERCP surgery has evolved from a pure diagnostic technique to a primarily treatment-oriented comprehensive minimally invasive technique. It is an important means of clinical diagnosis and treatment of biliary and pancreatic diseases.
Cholangiography
Sphincterotomy and dilation of the ampulla of Vater
Endoscopic extraction of bile duct and pancreatic duct stones
Dilation of bile duct and pancreatic duct strictures
Nasobiliary and nasopancreatic drainage procedures
Insertion of bile duct and pancreatic duct stents
Minimally invasive, little patient discomfort, and complete cure without the need for surgical laparotomy.
Mature technology, high success rate, and few complications.
Short treatment time, low cost, and rapid recovery: Patients can be physically active after the surgery, resume eating the next day, and generally only need to stay in the hospital for 3-5 days, with treatment costs and hospital stays only half to one-third of traditional surgical procedures.
Broad indications, not limited by adhesive cholangitis after multiple surgeries or elderly frailty, and ERCP equipment technology reduces the risk of treatment and is more conducive to patient recovery.
Jaundice caused by biliary obstruction.
Clinical, laboratory, or imaging support for pancreatic or biliary diseases (such as stones, tumors, sclerosing cholangitis, etc.).
Pancreatic diseases: pancreatic tumors, chronic pancreatitis, pancreatic cysts, etc.
Pancreatitis of unknown cause.
Strictly adhere to the indications for endoscopic examination.
Before the surgery, the patient and family must sign an informed consent form informing them of the risks and possible complications of the operation, as well as the operation process, benefits, and potential complications.
Fasting for 4-6 hours before the surgery.
Preoperative medication: atropine 20mg, diazepam 5mg, and pethidine 50mg.
Understand the patient's coagulation status, stop using antiplatelet drugs and anticoagulants one week in advance.
Check amylase in the blood at 12 and 24 hours after the surgery, and urine amylase after 24 hours. Continue to check if it becomes elevated and return to normal.
After 24-48 hours of fasting, gradually transition from low-fat liquid diet to normal diet based on amylase levels.
Observe the nasobiliary drainage for color, quality, and quantity, which can reach 500-1000ml per day and gradually decrease. Be wary of the drainage tube blockage or placement in the pancreatic duct.