 English
English 한국어
한국어 français
français Deutsch
Deutsch Español
Español русский
русский português
português العربية
العربية ไทย
ไทย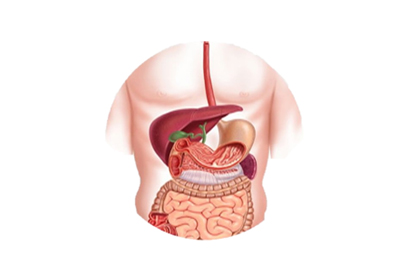

Address
1st & 2nd Floor, 10 Building, 18 Huashan Rd., Changzhou, Jiangsu province, China

Endoscopic nasobiliary drainage is a technique used to prevent post-ERCP and stone removal procedures from causing cholangitis and pancreatitis. The procedure involves the placement of a drainage tube into the predetermined location of the bile duct using endoscopic retrograde cholangiopancreatography (ERCP). The tube passes through the duodenum, stomach, esophagus, and is brought out through the nostrils to form nasobiliary drainage. Proper care and management of the nasobiliary drainage tube post-procedure is critical to its success in preventing complications. Improper observation and management of nasobiliary drainage can even pose a risk to the patient's life.
The ERCP equipment requires the highest level of skilled assistance from nurses in any endoscopic surgery. Firstly, nurses must monitor and observe the patient's vital signs constantly, enabling the operating doctor to solely focus on the operation, while at the same time providing feedback in order to take appropriate action quickly. Nurses must also effectively calm and educate patients who are in sedation before and during the operation, reducing their anxiousness and increasing their cooperation.
The assistance provided by the nurse during the operation is particularly crucial. The difference between having an experienced nurse and a novice nurse assist the operation doctor is huge. An experienced nurse can even guide a beginner doctor in performing ERCP surgery. Experienced nurses will make judgments regarding the direction and the shape of the bile duct, and observe the doctor's process of inserting the catheter. Once the catheter is in position, they will quickly insert the guide wire and proceed cautiously. The guide wire will enter the common bile duct and make way for segmented fluoroscopy, allowing doctors to understand the nature of obstructions and the degree of dilation in the bile duct. For patients with high bile duct pressure, bile should be drawn before fluoroscopy to avoid complications.
During the operation, nurses must cooperate closely with the doctors. After the guide wire has been inserted into the desired location, and the nasobiliary drainage tube is in its ideal position, all of the guide wire must be removed. The nasobiliary drainage tube should avoid any sharp bends, and should be positioned at the lesser curvature of the stomach, forming the ideal loop in the duodenum and stomach. Once contrast medium has been injected through the nasobiliary drainage tube, the position of the tube in the head of the bile duct must be further determined. If it is not ideal, the ERCP guidewire must be reinserted for adjustment, and the mouth should also be checked for any twists or folds. We have experienced instances where nurses have not checked carefully which led to twists or folds in the mouth of the nasobiliary drainage tube, causing ineffective bile drainage and worsening the condition after surgery.
Post-operative care of nasobiliary drainage following ERCP surgery is particularly important, but is usually completed by ward nurses. After returning from the endoscopic center to the ward, medical staff will assist the patient in finding a comfortable position, provide psychological comfort, and monitor changes in vital signs and the nature, color, and amount of bile drainage fluid. Typically, the volume of bile drainage will reduce from greater to lesser, and the color from dark to light, usually exceeding 300ml/day. Meanwhile, the patient's abdominal pain, bloating, and fever will subside, and jaundice will gradually decrease, indicating ideal drainage. Patients who require flushing of the nasobiliary drainage tube should use physiological saline solution according to the instructions, and the amount of fluid injected each time should not exceed 20ml. Before flushing, the same amount of bile should be withdrawn at a steady pace to avoid excessive pressure in the bile duct, which may induce or exacerbate infection. If drainage volume suddenly decreases, or drainage fluids change from bile to gastric contents, the possibility of the nasobiliary drainage tube dislocating must be considered, and an X-ray examination is necessary to check and reposition the tube, if needed. When the patient's bile drainage volume, color, body temperature, blood test results, and lipase levels have recovered to normal, and abdominal distension has eased, the tube may be removed.
ERCP surgery requires a surgical team, and besides the operation doctor's technical skills, a preoperative observation, intraoperative assistance, and postoperative nursing care by endoscopic nursing staff is necessary to reduce complications after the procedure. Nurses should focus on psychological care prior to ERCP, patiently introducing the operating steps and precautions to the patient, and relieving any anxiety and fear the patient may have, thus improving the patient's participation in the treatment process.