 English
English 한국어
한국어 français
français Deutsch
Deutsch Español
Español русский
русский português
português العربية
العربية ไทย
ไทย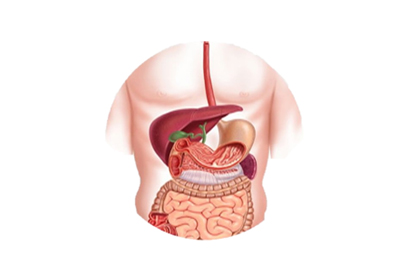

Address
1st & 2nd Floor, 10 Building, 18 Huashan Rd., Changzhou, Jiangsu province, China

ERCP, namely endoscopic retrograde cholangiopancreatography, is to insert a duodenoscope into the descending part of the duodenum, find the main papilla of the duodenum, insert a catheter into the opening of the papilla from the biopsy duct, inject a contrast agent, and take X-rays. slice to show the pancreaticobiliary duct. The success rate of ERCP has been increasing year by year, reaching about 90% at present, and it is currently recognized as the gold standard for diagnosing pancreaticobiliary diseases. On the basis of ERCP equipment, interventional treatments such as duodenal sphincterotomy (EST), endoscopic nasal bile drainage, and endoscopic bile internal drainage can be performed. Because no surgery is required and the trauma is small, hospitalization is possible. The time is also greatly shortened, which is very popular among patients.
1. Unexplained obstructive jaundice with suspected extrahepatic biliary obstruction.
2. Those who are suspected to have various biliary tract diseases such as stones, tumors, sclerosing cholangitis and other unknown diagnoses.
3. Suspected congenital biliary abnormalities or recurrence of symptoms after cholecystectomy.
4. Pancreatic diseases: pancreatic tumors, chronic pancreatitis, pancreatic cysts, etc.
Although there are many advantages in using ERCP equipment for surgery, such as ERCP balloon dilation, it should be noted that ERCP surgery cannot be performed if there are the following contraindications.
1. Severe cardiopulmonary or renal insufficiency.
2. Acute pancreatitis or acute exacerbation of chronic pancreatitis.
3. Severe biliary tract infection.
4. Allergy to iodine contrast agent.
You will be asked to sign an informed consent form confirming that you understand the risks and benefits of the procedure and authorizing your doctor to perform the procedure. The upper gastrointestinal tract must be emptied, and no food or drink is allowed for 8 hours before the ERCP devices. Before and after surgery, there are some restrictions on the use of the drug; especially in patients with hypertension, diabetes and blood thinners or patients with coagulation abnormalities.
The endoscopist needs to work with the anesthesiologist to apply local anesthetics to the patient's throat to paralyze and relieve the vomiting response of the pharynx. General anesthesia is also often applied, and patients are required to wear mouth pads to protect their teeth and endoscopes. The vital signs of the patient were also closely monitored throughout the operation. Operating time depends on the complexity of the procedure. The duodenoscope passes through the patient's mouth, through the esophagus and stomach to the duodenum. Then, endoscopic gas insufflation dilates the lumen of the duodenum for observation. ERCP guide wire and catheter are inserted through the opening of the nipple, combined with X-ray machine scanning, guide wire and catheter injection of contrast agent, determine the location of the lesion, and enter the pancreatic duct or bile duct accordingly. After insertion of the intended pancreatic/biliary duct, identify the problem and provide appropriate treatment.
If the stone is identified as being within the pancreatic or biliary tree, it can be removed by cutting the internal papillary sphincter muscle, which is called a sphincterotomy. A balloon is used to drag and clear the bile duct, pulling the stone out of the duct and into the duodenum. The cleared stones can be safely passed out of the body with feces.
If obstruction or suspicious tissue is found, appropriate sample tissue can be taken and sent to the pathology department for examination. When the tumor causes bile duct obstruction and drainage is required, if it is a malignant disease, a metal stent can be implanted; if the nature of the obstruction is unknown, a plastic stent can be implanted to bridge the obstructed bile duct and restore drainage to the duodenum. According to different conditions, it may also involve more treatment of bile duct stricture and dilatation, stone crushing in bile duct, bile duct and pancreatic duct brushing, insertion of nasobiliary drainage tube, etc.
Compared with conventional endoscopic diagnosis and treatment, the risk of surgery using endoscopy accessories is more invasive, but it is much less traumatic than surgery. most common complication is pancreatitis, and patients need to be hospitalized for a few days. Other less common complications include: bleeding, infection, perforation and even death.